Cancer describes a set of diseases in which normal cells in the body, through a series of genetic changes, become abnormal and lose the ability to control their growth.
As cancers – also known as malignancies – grow, they invade the tissues around them (local invasion).
They may also spread to other locations in the body via the blood vessels or lymphatic channels where they may implant and grow (metastases).
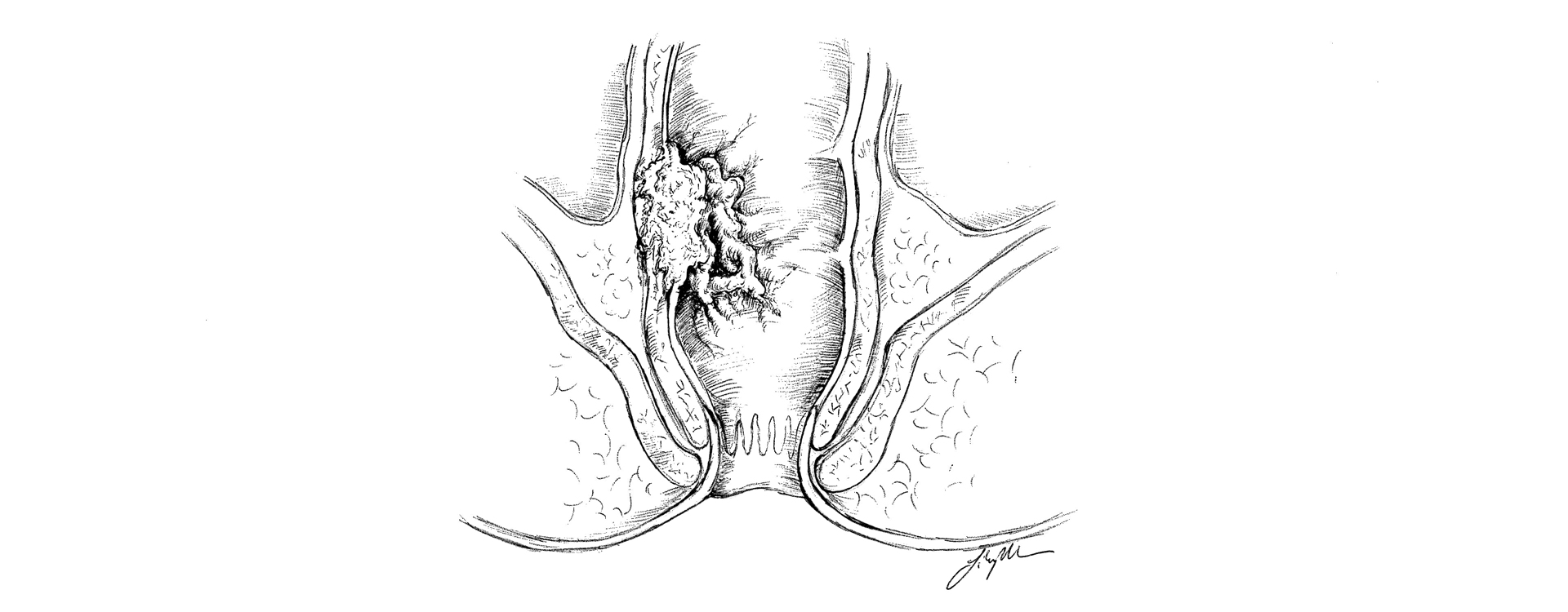
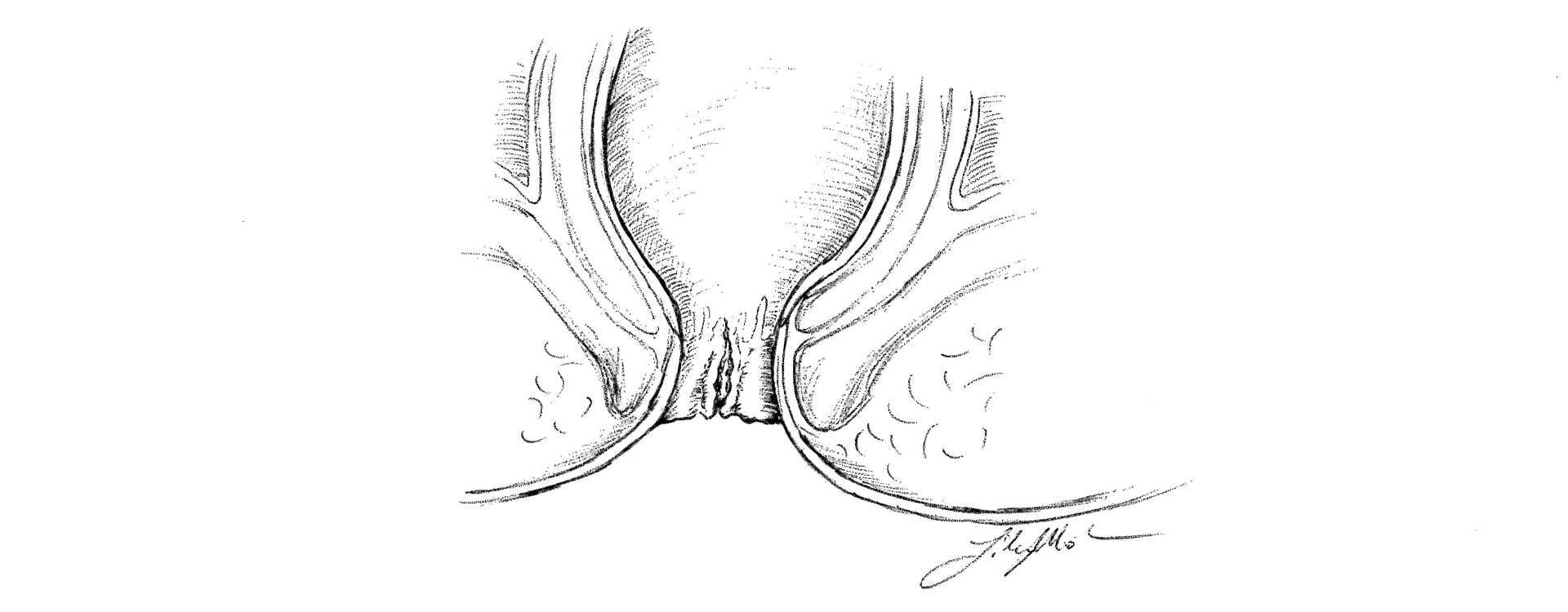
The anus or anal canal is the passage that connects the rectum, or last part of the large intestine, to the outside of the body.
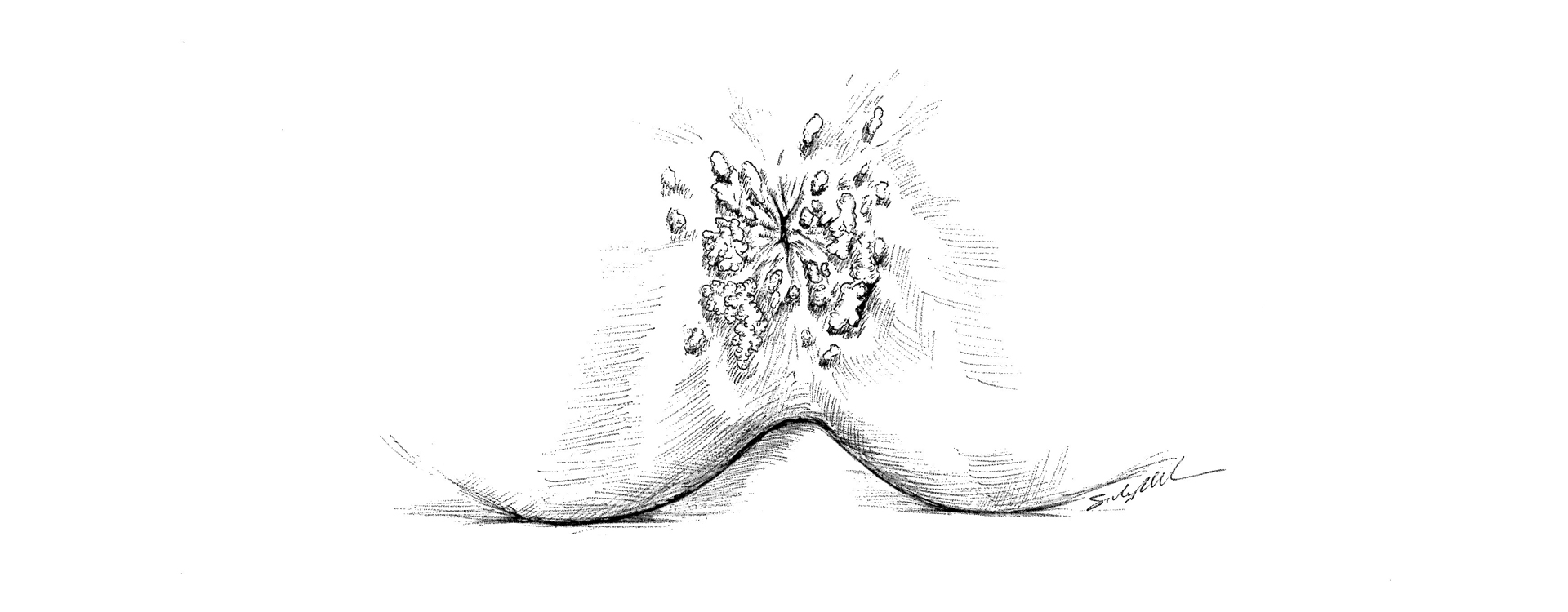
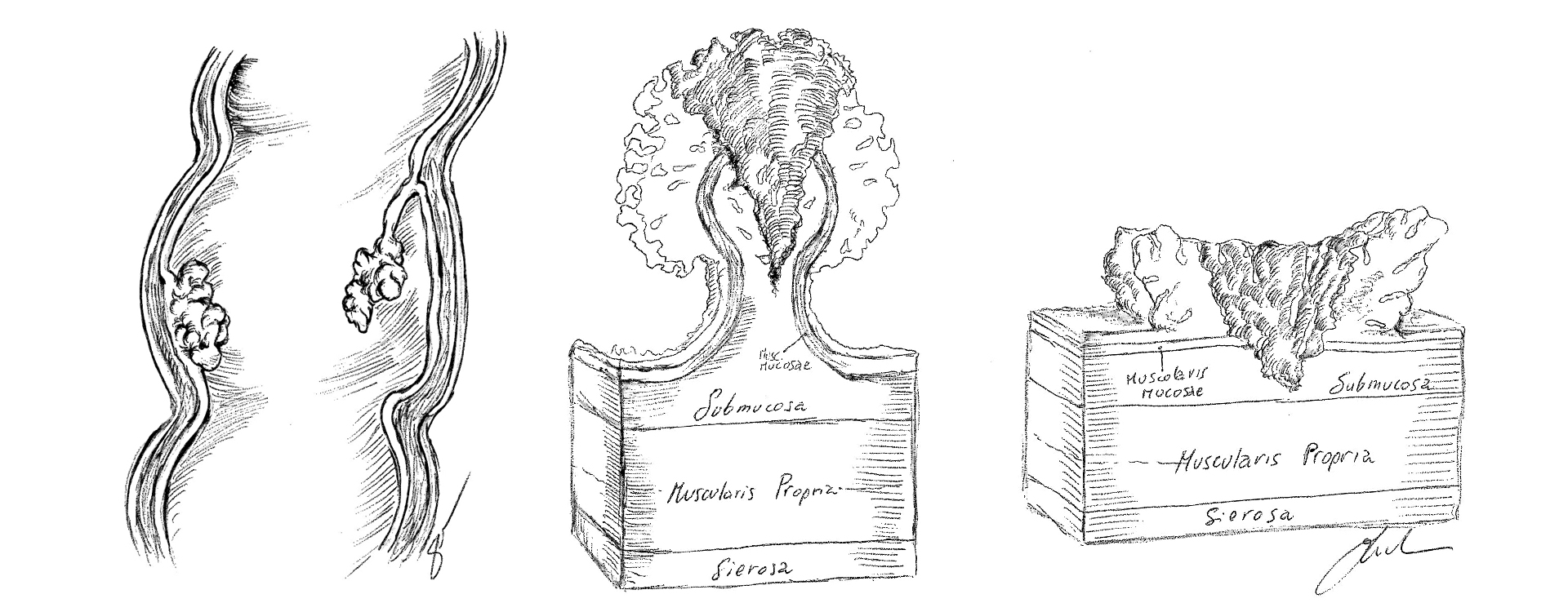
Anal cancer arises from the cells around the anal opening or in the anal canal just inside the anal opening.
Anal cancer is often a type of cancer called squamous cell carcinoma.
Other rare types of cancer may also occur in the anal canal and these require consultation with your physician or surgeon to determine the appropriate evaluation and treatment.
Cells that are becoming malignant or premalignant, but have not invaded deeper into the skin, are referred to as high-grade anal intraepithelial neoplasia or HGAIN (previously referred to by a number of different terms, including high grade dysplasia, carcinoma-in-situ, anal intra-epithelial neoplasia grade III, high-grade squamous intraepithelial lesion, or Bowen's disease).
While this condition is likely a precursor to anal cancer, this is not anal cancer and is treated differently than anal cancer.
Your physician or colon and rectal surgeon can help clarify the differences.
How common is anal cancer?
Anal cancer is fairly uncommon, and accounts for about 1-2% of cancers affecting the intestinal tract.
Approximately one in 600 men and women will get anal cancer in their lifetime (this can be compared to 1 in 20 men and women who will developed colon and rectal cancer in their lifetime).
Almost 6,000 new cases of anal cancer are now diagnosed each year in the U.S., with about 2/3rds of the cases in women.
Approximately 800 people will die of the disease each year.
Unlike some cancers, the numbers of patients that develop anal cancer each year is slowly increasing, especially in some higher risk groups (see below).
Who is at risk?
A risk factor is something that increases a person's chance of getting a disease.
Anal cancer is commonly associated with infection with the human papilloma virus (HPV), but some anal cancers develop without this infection being present.
HPV can also cause warts in and around the anus as well as genital warts (on the penis in men and the vagina or cervix in women), but warts do not have to be present for anal cancer to develop.
HPV is also associated with an increased risk of cervical and vaginal or vulvar cancer in women, penile cancer in men, as well as with some head and neck cancers in men and women.
Having some of these cancers, especially cervical or vulvar cancer (or even pre-cancerous change in the cervix or vulva), can put people at increased risk for anal cancer – likely from the association with HPV infection.
Additional risk factors for anal cancer include:
- age (while most of the cases of anal cancer develop in people over age 55, 1/3rd of the cases occur in patients that are younger than that)
- anal sex (people participating in anal sex, both men and women, are at increased risk)
- sexually transmitted diseases (patients with multiple sex partners are at higher risk of getting sexually transmitted diseases like HPV and HIV and are, therefore, at an increased risk of developing anal cancer)
- smoking (harmful chemicals from smoking increases the risk of most cancers, including anal cancer)
- immunosuppression (people with weakened immune systems, such as transplant patients who must take drugs to suppress their immune systems and patients with HIV infection, are at higher risk)
- chronic local inflammation (people with long-standing anal fistulas or open wounds in the anal area are at a slightly higher risk)
- pelvic radiation (people who have had pelvic radiation therapy for rectal, prostate, bladder or cervical cancer are at increased risk)
Can anal cancer be prevented?
Few cancers can be totally prevented, but the risk of developing anal cancer may be decreased significantly by avoiding the risk factors listed above and by getting regular checkups.
Avoiding anal sex and infection with HPV and HIV can reduce the risk of developing anal cancer.
Using condoms whenever having any kind of intercourse may reduce, but not eliminate, the risk of HPV infection.
Smoking cessation lowers the risk of many types of cancer, including anal cancer.
Vaccines against infection with certain types of HPV, especially in high-risk patients (see risk factors listed above), may also decrease the risk of developing anal cancer (in men and women).
People who are at increased risk for anal cancer based on the risk factors listed above should talk to their doctors about consideration for anal cancer screening.
This can include anal cytology or Pap tests (much like the Pap tests women undergo for cervical cancer screening).
Early identification and treatment of premalignant lesions in the anus may also prevent the development of anal cancer.
What are the symptoms of anal cancer?
Although 20% of anal cancers may be asymptomatic, many cases of anal cancer can be found early because they form in a part of the digestive tract that a doctor can see and reach easily.
Anal cancers may cause symptoms such as:
- bleeding from the rectum or anus
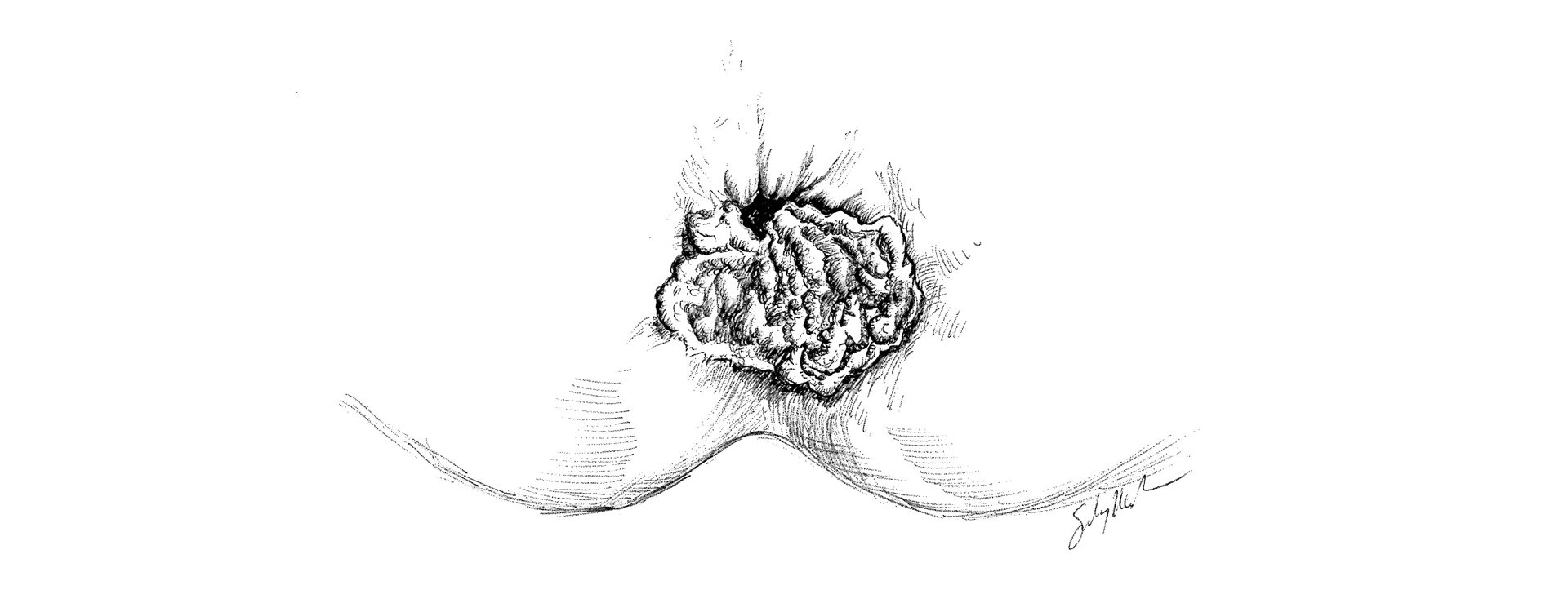
- the feeling of a lump or mass at the anal opening
- persistent or recurring pain in the anal area
- persistent or recurrent itching
- change in bowel habits (having more or fewer bowel movements) or increased straining during a bowel movement
- narrowing of the stools
- discharge or drainage (mucous or pus) from the anus
- swollen lymph nodes (glands) in the anal or groin areas
These symptoms can also be caused by less serious conditions such as hemorrhoids, but you should never assume this.
If you have any of these symptoms, see your doctor or colon and rectal surgeon.
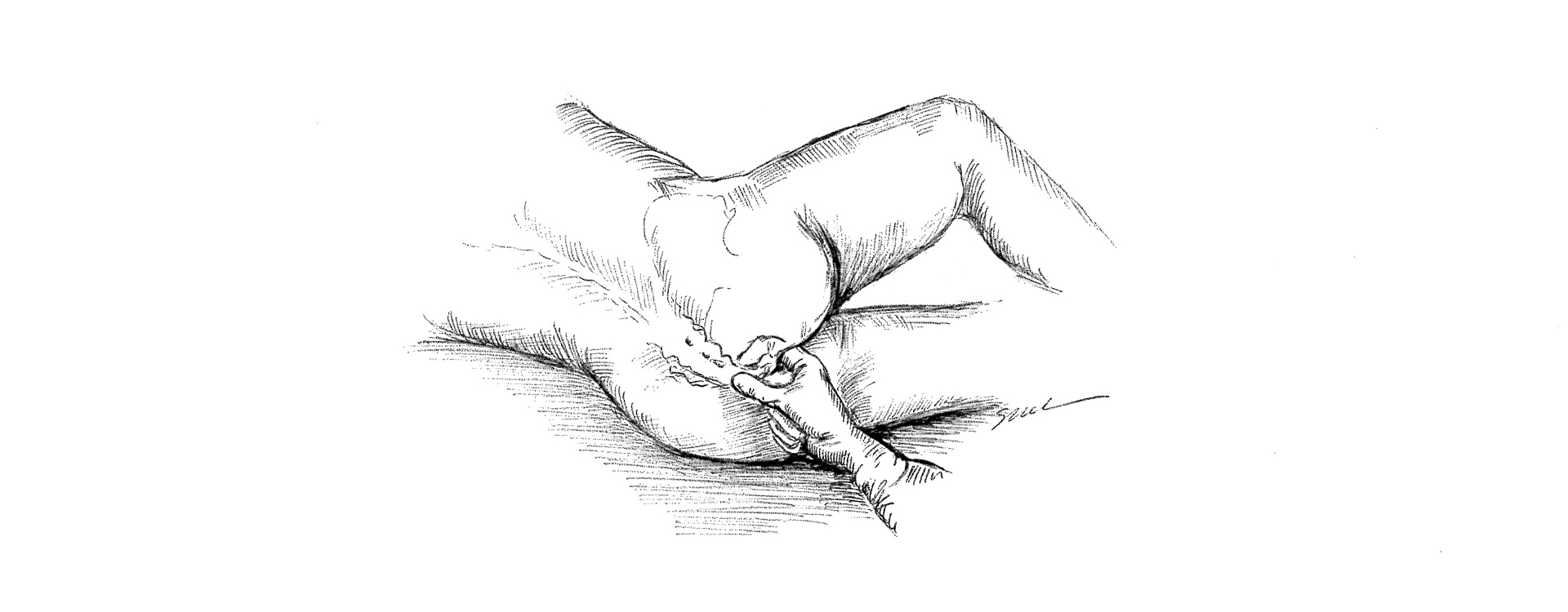
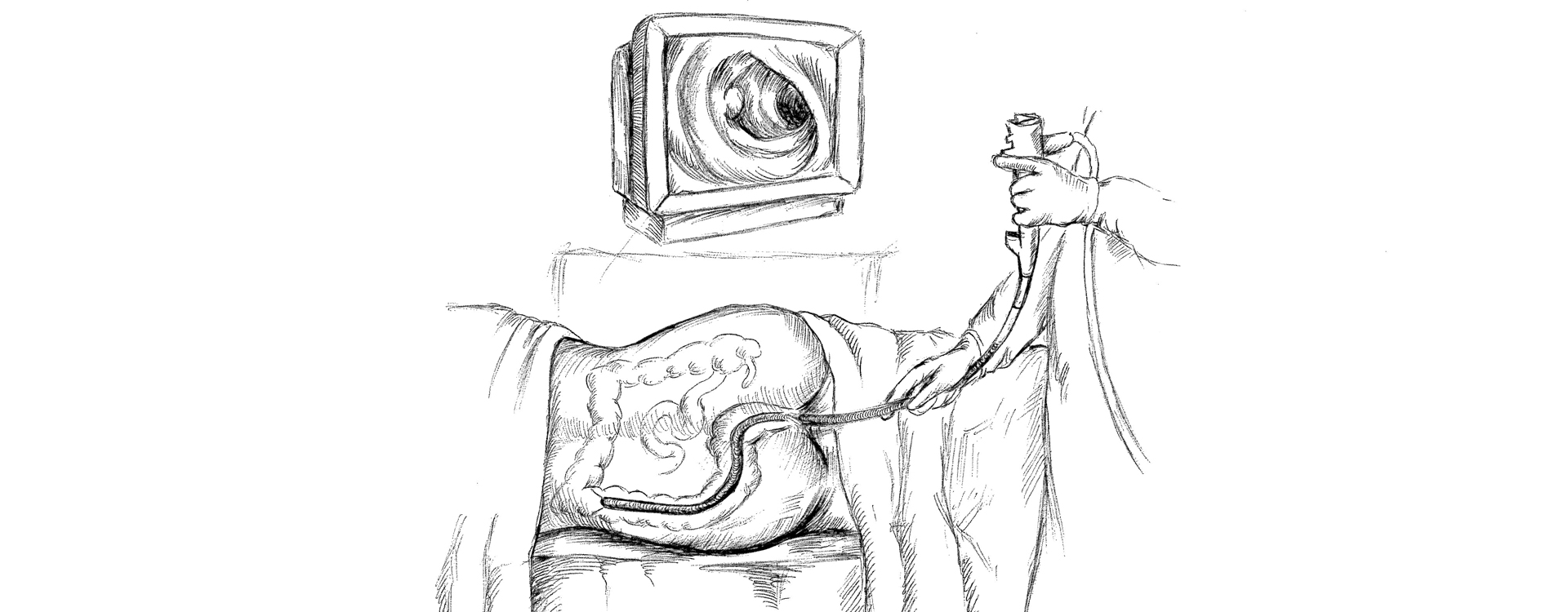
How is anal cancer diagnosed?
Anal cancer is usually found on examination of the anal canal because of the presence of symptoms listed above, on routine yearly physical exams by a physician (rectal exam for prostate check or at the time of a pelvic exam), or on screening tests such as those recommended for preventing or diagnosing colorectal cancer (for example: colonoscopy or lighted scope exam of the colon and rectum or yearly stool blood tests).
Anoscopy, or examination of the anal canal with a small, lighted scope, may be performed as well to assess any abnormal findings.
If an abnormal area in the anal canal is identified based on the doctor's exam, a biopsy will be performed to determine the diagnosis.
If the diagnosis of anal cancer is confirmed, additional tests to determine the extent of the cancer may be recommended, which may include ultrasounds, Xrays, CT scans, and/or PET scans.
How are anal cancers treated?
Treatment for most cases of anal cancer is very effective in curing the cancer.
There are 3 basic types of treatment used for anal cancer:
- surgery (an operation to remove the cancer)
- Radiation therapy (high-dose x-rays to kill cancer cells)
- Chemotherapy (giving drugs to kill cancer cells)
Combination therapy including radiation therapy and chemotherapy is now considered the standard treatment for most anal cancers.
Occasionally, a very small or early tumor may be removed surgically (local excision) without the need for further treatment and with minimal damage to the anal sphincter muscles that are important for bowel control.
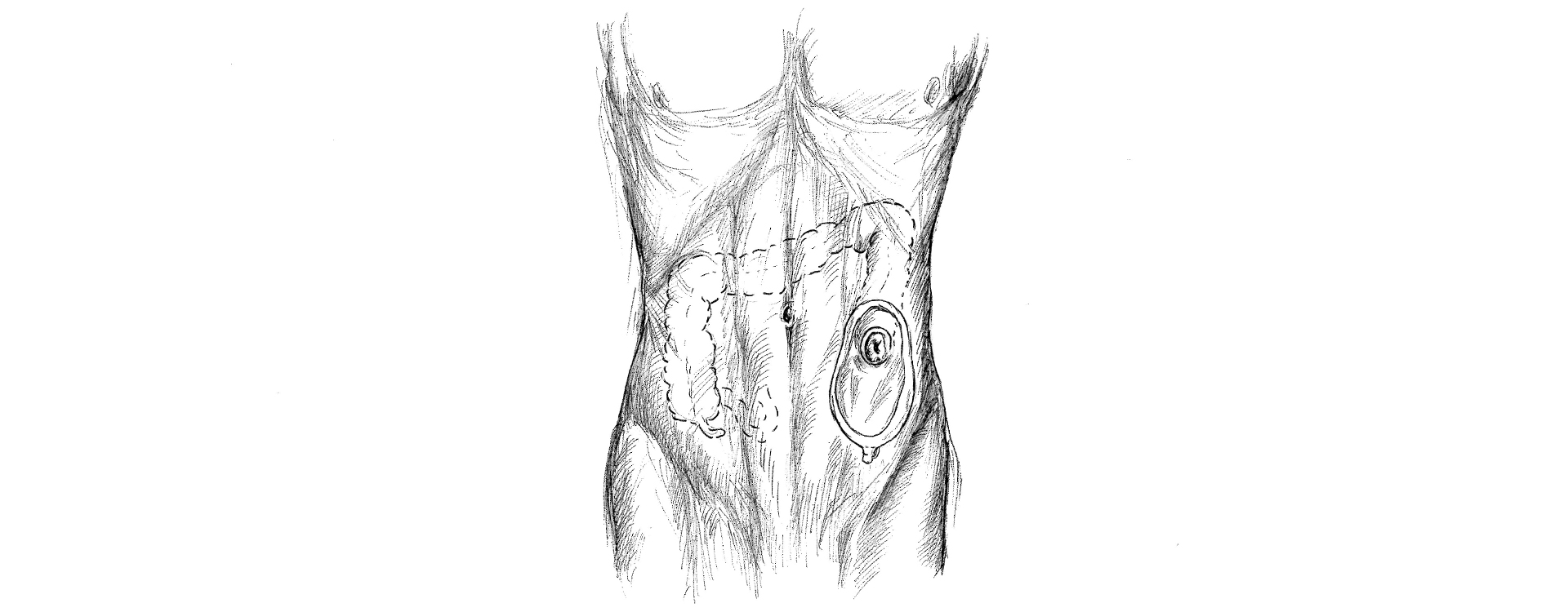
On occasion, more major surgery to remove the anal cancer is needed, and this requires the creation of a colostomy where the bowel is brought out to the skin on the belly wall where a bag is attached to collect the fecal matter.
Will I need a colostomy?
The majority of patients treated for anal cancer will not need a colostomy.
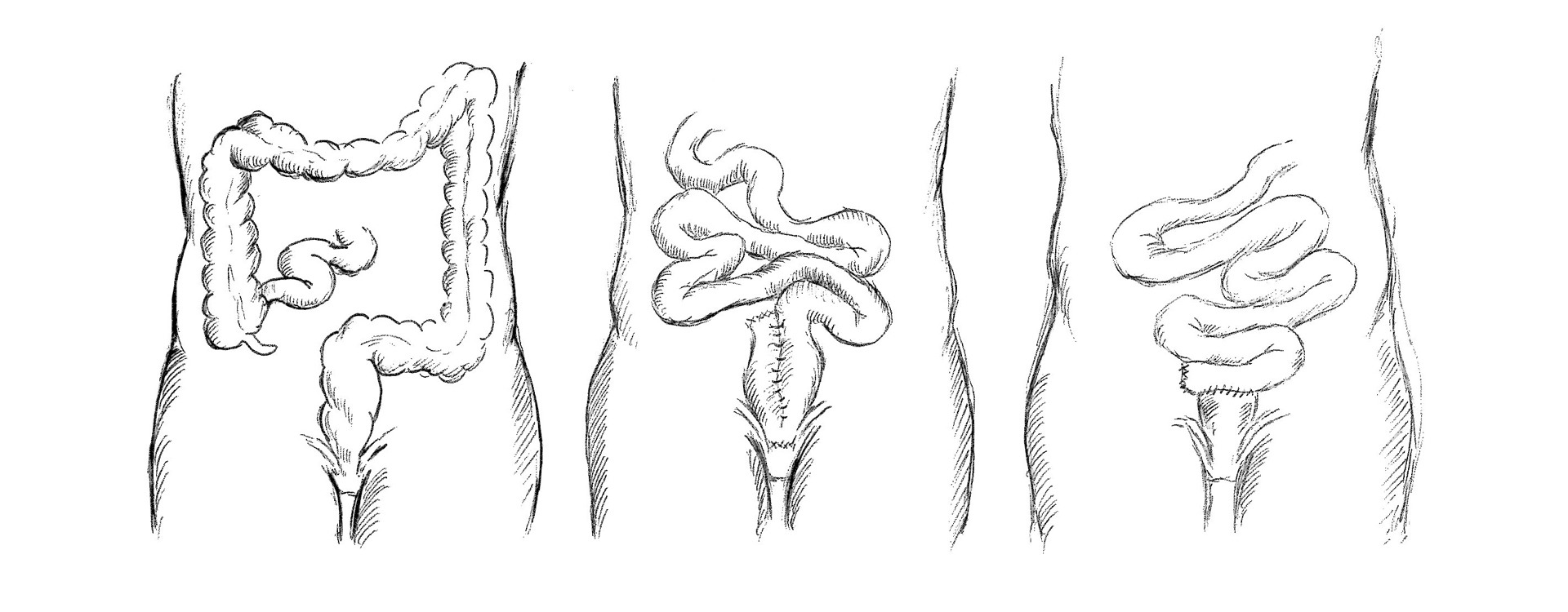
If the tumor does not respond completely to combination therapy, if it recurs after treatment, or if it is an unusual type of anal cancer, removal of the rectum and anus and creation of a permanent colostomy may be necessary.
This operation is known as an abdominoperineal resection (APR).
What happens after treatment for anal cancer?
Follow-up care to assess the results of treatment and to check for recurrence is very important.
Most anal cancers are cured with combination therapy and/or surgery, so you should report any symptoms or problems to your doctor or surgeon right away.
In addition, many tumors that recur may be successfully treated with surgery if they are caught early.
A careful examination by an experienced physician or colon and rectal surgeon at regular intervals is the most important method of follow-up.
Additional studies, such as certain types of scans (for example, CT or MRI) or ultrasounds, may also be recommended.
Conclusion
Anal cancers are unusual tumors arising from the skin or lining of the anal canal.
As with most cancers, early detection is associated with excellent survival.
Most tumors are well-treated with combination chemotherapy and radiation.
Recurrences, treatment failures, and advanced disease may require surgery.
Follow the recommended screening examinations for anal and colorectal cancer and consult your doctor or colon and rectal surgeon early when any concerning symptoms occur.